
Transplant Procedure
 The liver transplant operation involves removal of the unhealthy liver of the patient and replacing it with the healthy liver. The operation to remove the diseased liver of the patient (recipient hepatectomy) is technically challenging because the liver is firmly attached to surrounding organs with tissues containing many thin walled blood vessels (collaterals) with blood under a lot of pressure (portal hypertension). A lot of bleeding can occur during this phase of surgery and enough blood should be arranged to replace the losses. The entire diseased liver must be removed in such a way that the main blood vessels and bile duct of the patient are preserved to be joined to those of the new liver.
The liver transplant operation involves removal of the unhealthy liver of the patient and replacing it with the healthy liver. The operation to remove the diseased liver of the patient (recipient hepatectomy) is technically challenging because the liver is firmly attached to surrounding organs with tissues containing many thin walled blood vessels (collaterals) with blood under a lot of pressure (portal hypertension). A lot of bleeding can occur during this phase of surgery and enough blood should be arranged to replace the losses. The entire diseased liver must be removed in such a way that the main blood vessels and bile duct of the patient are preserved to be joined to those of the new liver.
In living donor operation, the donor liver must be divided into two parts in such a way that not only the part which is left behind should be sufficient & working well in the donor but also the part of liver which is to be removed should be sufficient for the patient and work well after implantation. Both parts of the liver must have a blood supply into the liver as well as a way for the blood to leave the liver and a way for the bile to flow out of the liver. This is a much more difficult and challenging operation than removal of a portion of the liver for disease or cancer. In deceased (cadaveric) donor operation whole liver is removed.
Once removed, the donor liver (whole or portion of liver) is flushed with cold preservative solution and the blood vessels are prepared to be connected with those of the patient. This often involves extending the vessels of the donor liver with segments of vessels taken from the patients removed liver. The new liver is then implanted into the patient and all the blood vessels and the bile ducts joined to their counterparts in the patient. A Doppler ultrasound check is performed on the operation table to confirm that all the blood vessels are working well.
 Plain CT scan of Donor is done to assess amount of fat in liver
Plain CT scan of Donor is done to assess amount of fat in liver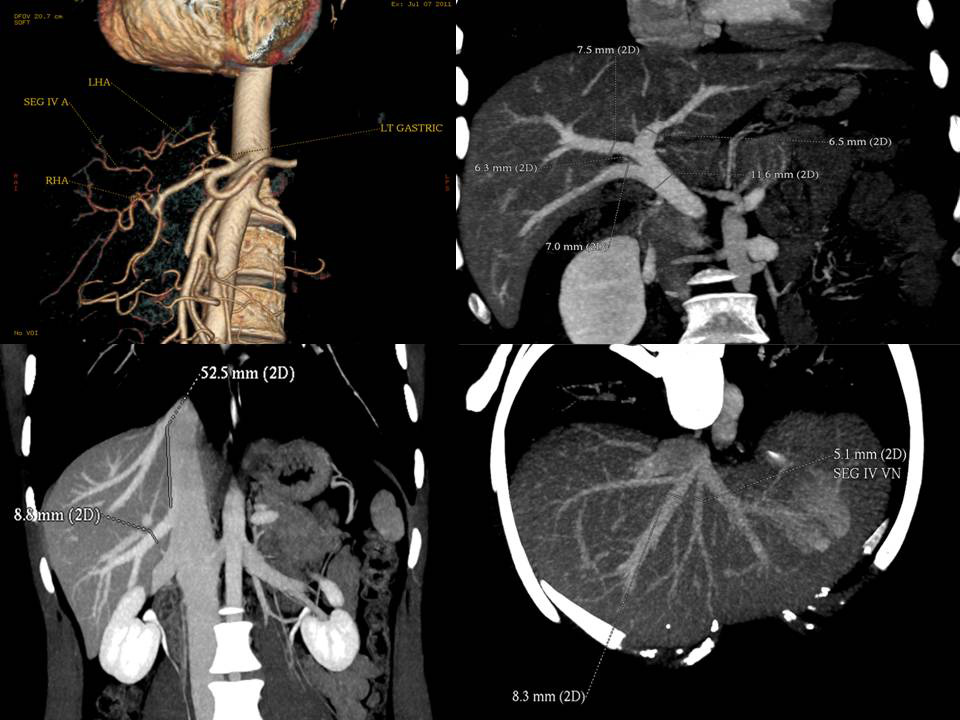 CT Angiogram of Donor gives detailed information about blood vessels in the donor and helps plan the operation.
CT Angiogram of Donor gives detailed information about blood vessels in the donor and helps plan the operation. MRCP of Donor gives us detailed idea about the anatomy of Bile ducts
MRCP of Donor gives us detailed idea about the anatomy of Bile ducts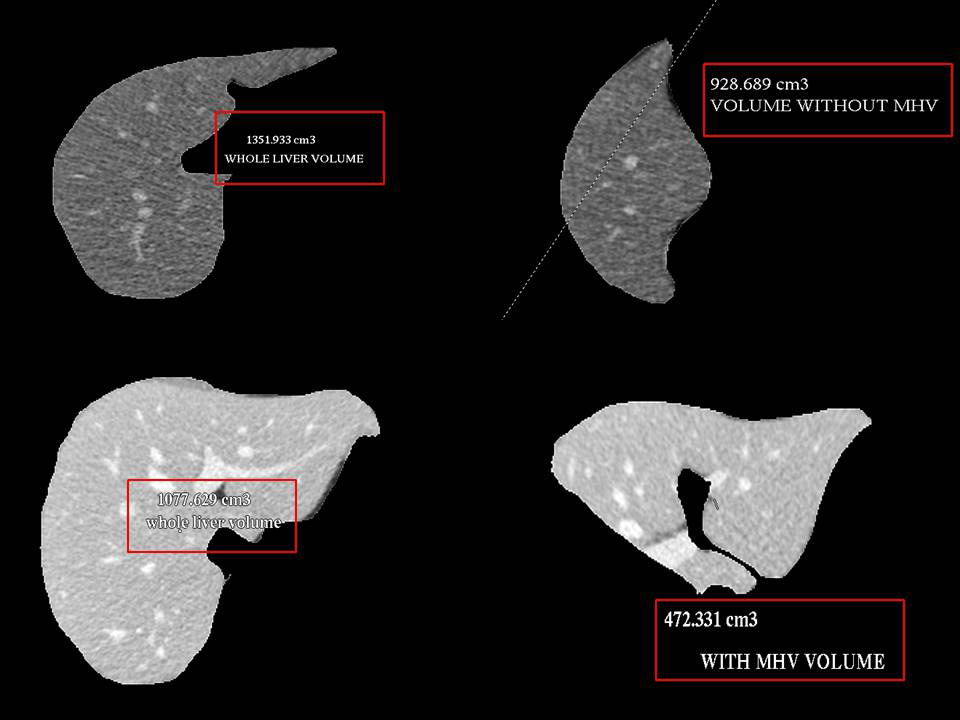 Volumetry of Donor Liver using CT scan gives an idea about the volumes of each side of liver
Volumetry of Donor Liver using CT scan gives an idea about the volumes of each side of liver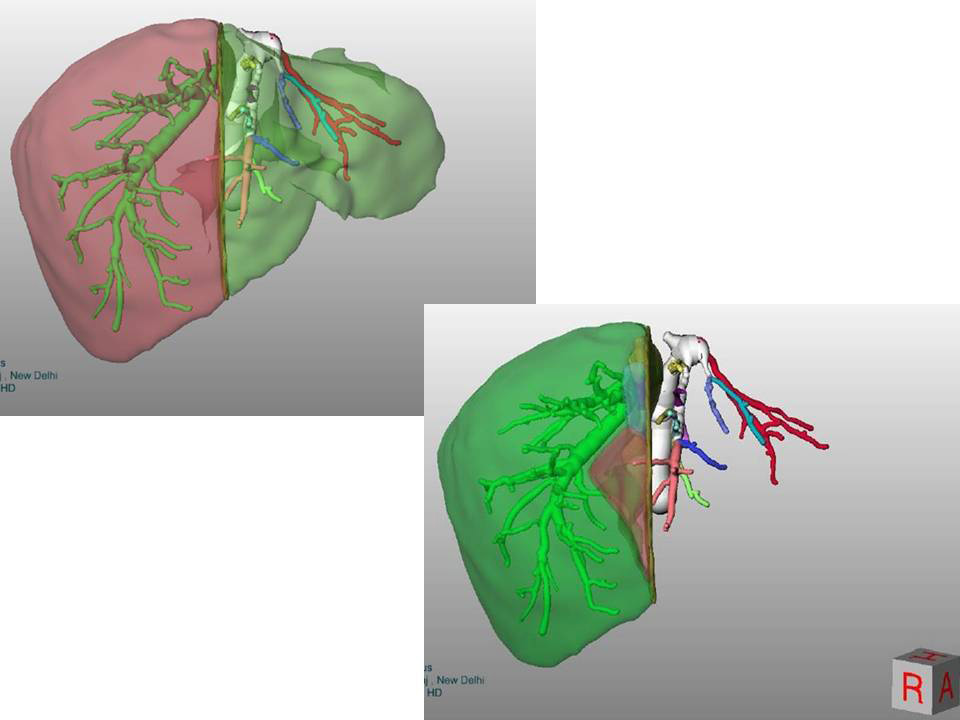 In complex cases sophosticated software helps in pre-surgery planning and virtual surgery
In complex cases sophosticated software helps in pre-surgery planning and virtual surgery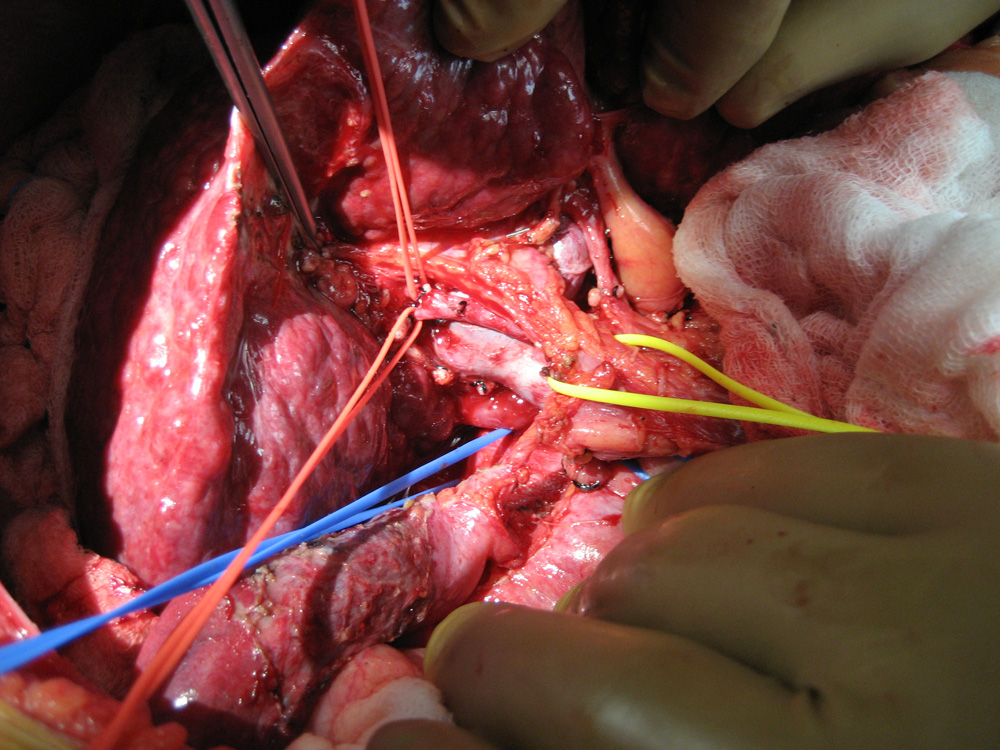 Blood vessels and bile duct of patient's liver being dissected
Blood vessels and bile duct of patient's liver being dissected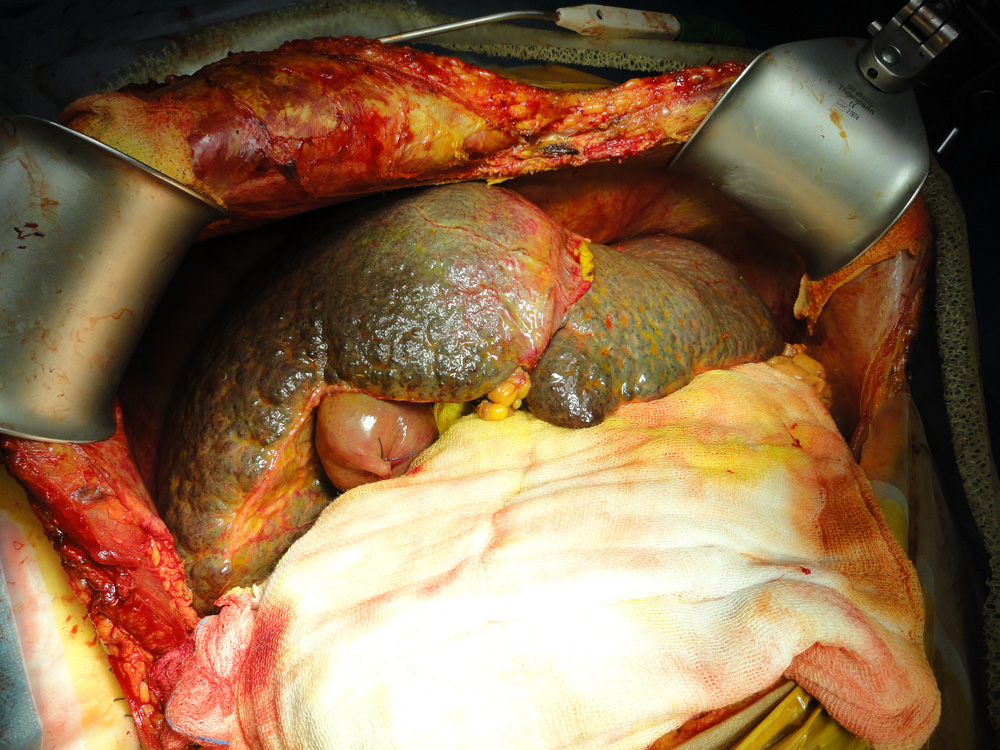 Diseased liver of the patient afflicted with Cirrhosis
Diseased liver of the patient afflicted with Cirrhosis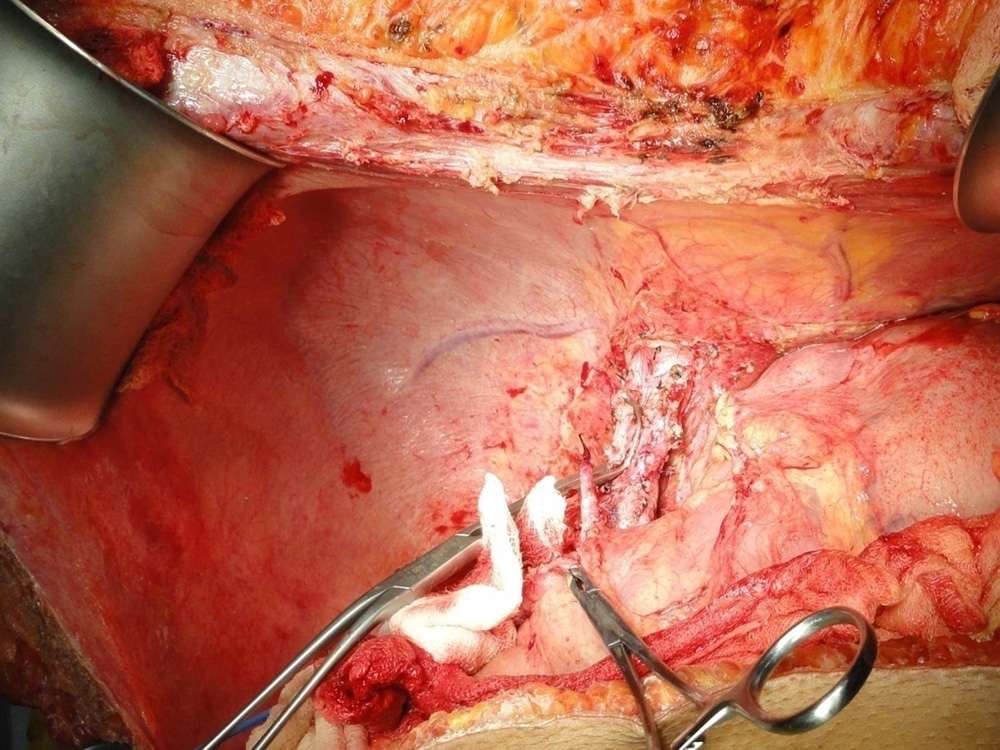 Diseased liver of the patient has been removed preseving blood vessels and bile duct
Diseased liver of the patient has been removed preseving blood vessels and bile duct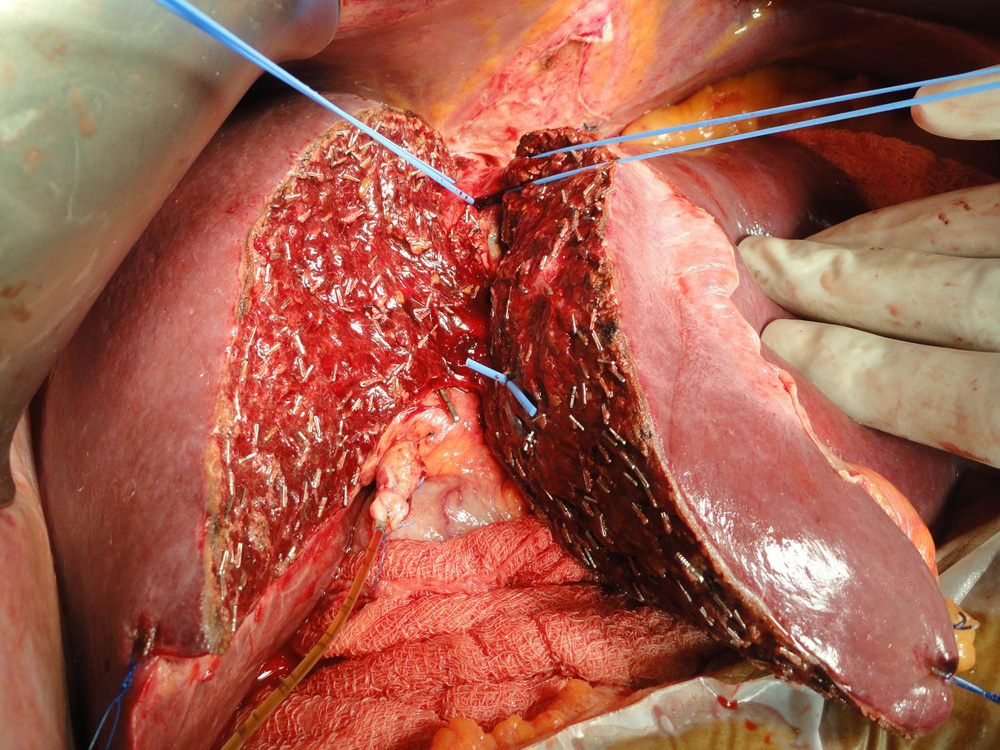 Donor liver is being split taking great care to preserve blood supply to both sides of the liver.
Donor liver is being split taking great care to preserve blood supply to both sides of the liver.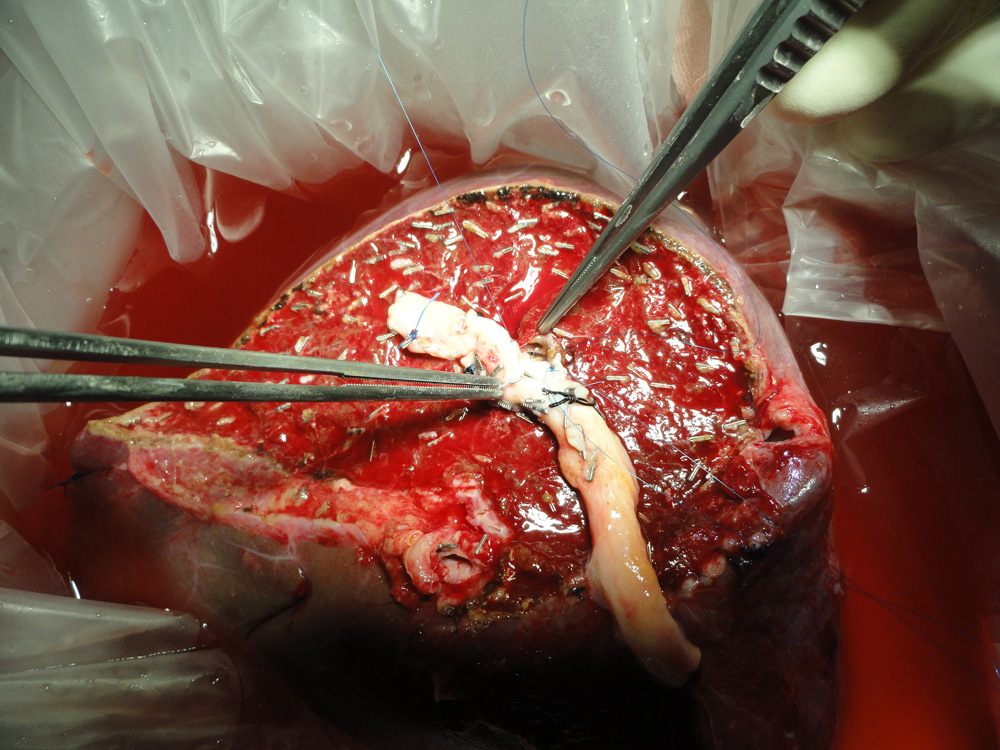 The portion of the donor liver which is going to be transplanted (in this case right lobe) is seen here
The portion of the donor liver which is going to be transplanted (in this case right lobe) is seen here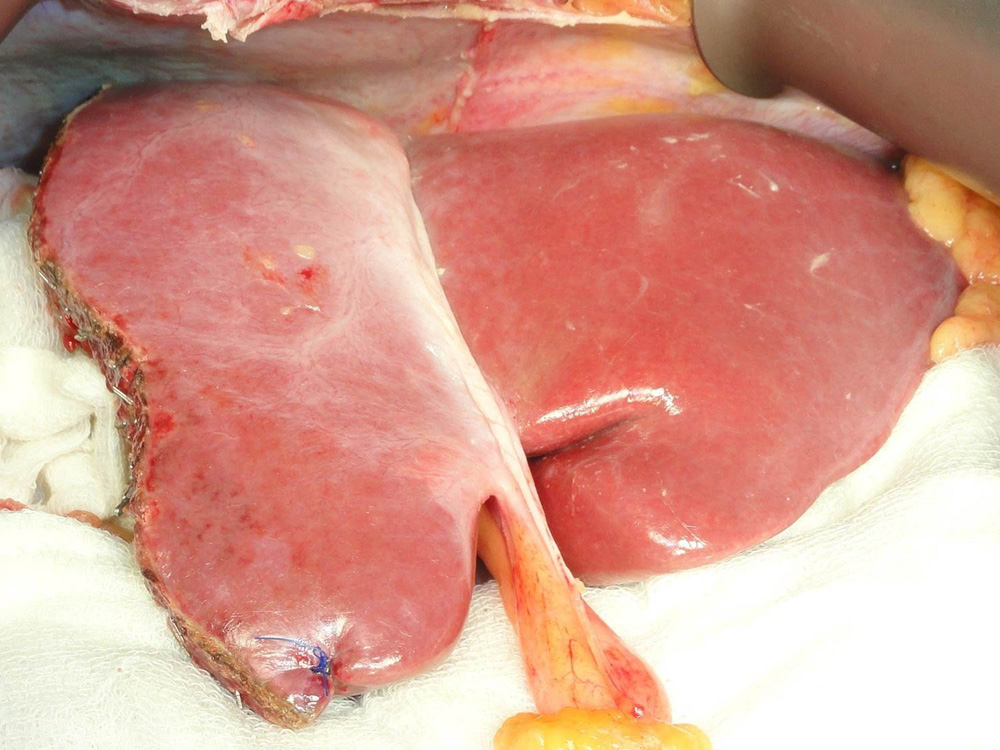 The remaining donor liver is seen after the portion to be transplanted has been removed.
The remaining donor liver is seen after the portion to be transplanted has been removed. The liver graft being modified during bench procedure
The liver graft being modified during bench procedure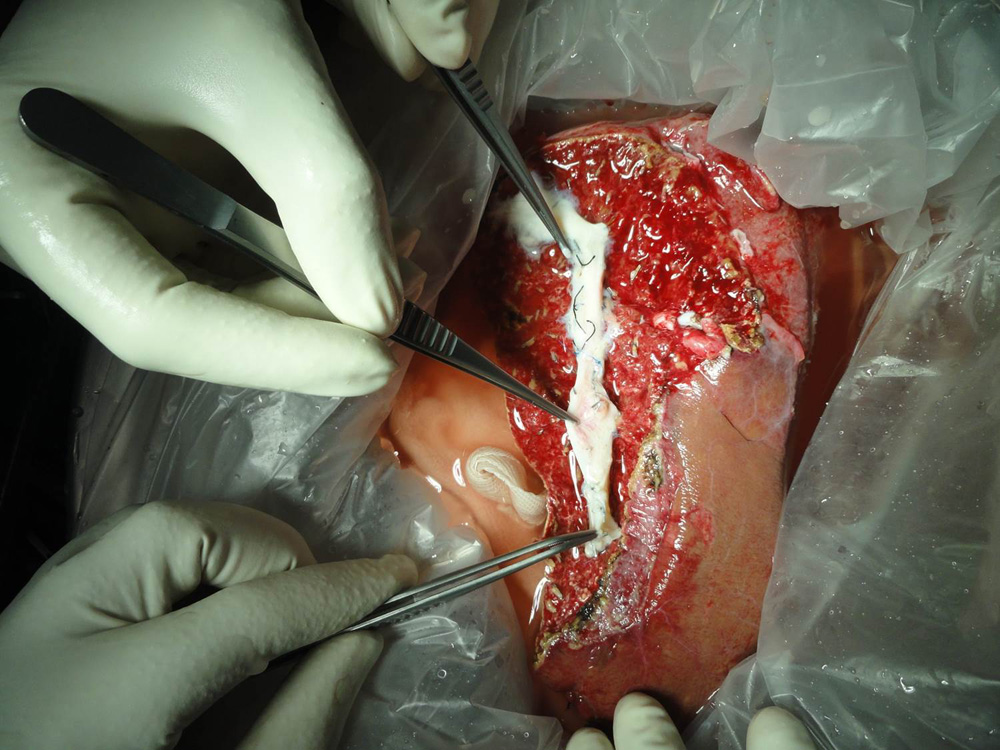 The middle hepatic vein is being reconstructed with a vein graft taken from the patient’s removed liver
The middle hepatic vein is being reconstructed with a vein graft taken from the patient’s removed liver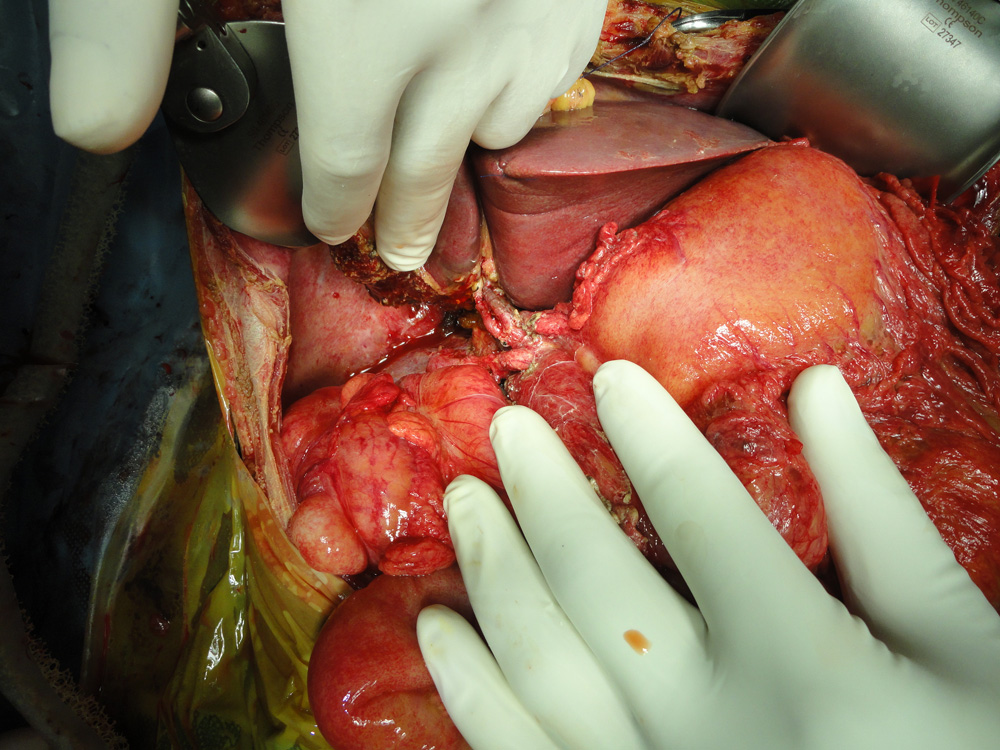 Left lobe liver transplant in a child. Two arteries have been reconstructed
Left lobe liver transplant in a child. Two arteries have been reconstructed Deceased donor (Cadaver) graft after retrieval
Deceased donor (Cadaver) graft after retrieval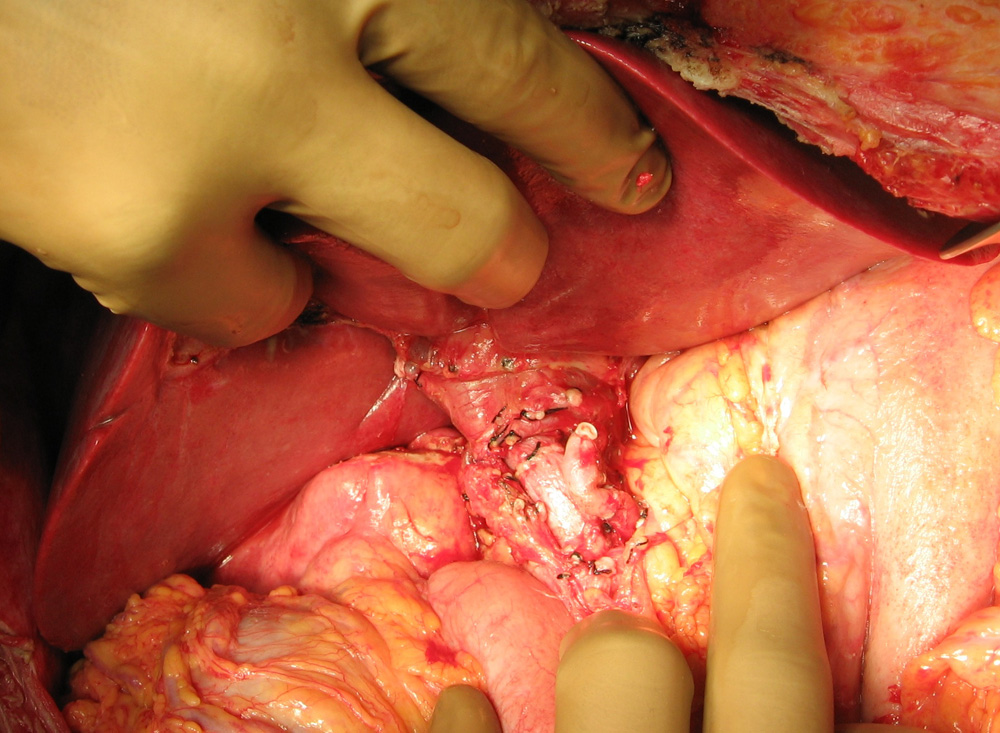 Deceased donor (Cadaver) graft after reperfusion
Deceased donor (Cadaver) graft after reperfusion Blood flow in the transplanted liver being verified using Doppler Ultrasound
Blood flow in the transplanted liver being verified using Doppler Ultrasound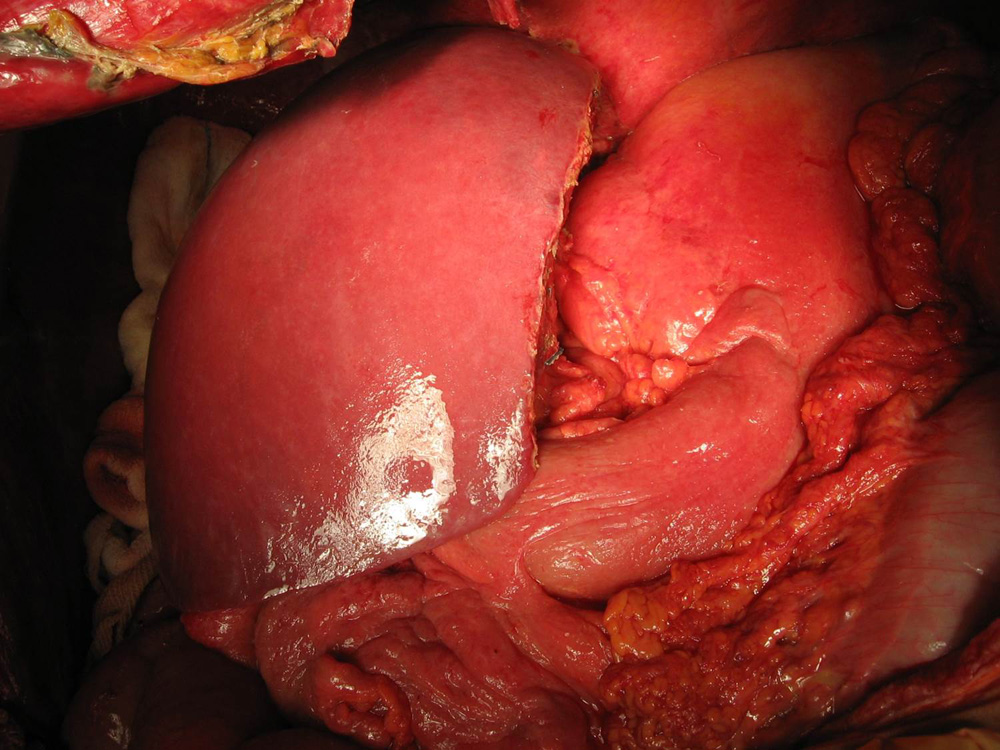 New Right-sided Liver at the completion of operation
New Right-sided Liver at the completion of operation